What Is the Clutter Image Rating Scale and How Do You Use It?
A humble set of photographs that changed how researchers, clinicians, and families talk about clutter — and why it’s more clever than it looks.
Let’s start with a problem that’s easy to overlook until you’re sitting right in the middle of it.
You’re a social worker. Or maybe you’re a therapist. Or perhaps you’re a grown child who’s just returned to your parent’s home after several years away, and you’re quietly alarmed by what you’re seeing. The living room is stacked with newspapers. The kitchen table has become a staging area for bags of things that haven’t been put away in what looks like a very long time. The bedroom, you suspect, is worse.
You want to know: how serious is this? Is this the beginning of a problem, or has it already crossed a line? And here’s the core challenge — the language we normally use to describe clutter is almost completely subjective. “Messy.” “Cluttered.” “A lot of stuff.” These words mean wildly different things to different people, in different homes, from different backgrounds. One person’s cozy collection is another person’s crisis. Without some shared framework, you’re basically guessing.
That’s exactly the problem that a team of researchers sat down to solve about two decades ago. And what they came up with was deceptively simple: photographs.
Nine photographs per room. Three rooms. A single number from 1 to 9. That’s the Clutter Image Rating Scale, and it’s become one of the most widely used assessment tools in the field of hoarding disorder research and treatment worldwide. It’s used in clinical offices across the United States, the United Kingdom, Canada, Europe, and beyond. It shows up in randomized controlled trials, CBT treatment protocols, community safety assessments, and social services intake procedures. And yes, anyone can use it — including you.
Let’s dig in.
The Origin Story: Why Words Weren’t Enough
Before we walk through how the scale works, it helps to understand why it had to be invented in the first place.
Prior to the Clutter Image Rating (CIR) being developed, clinicians and researchers who needed to assess the severity of hoarding had to rely primarily on self-report questionnaires. These are surveys where a person describes their own home, their own clutter levels, their own difficulty discarding things. In general, self-report measures work reasonably well for many psychological conditions. But for hoarding, they run into two very specific problems that make them unreliable on their own.
The first problem is over-reporting. Some people, particularly those who have sought out clinical help, may describe their clutter in more extreme terms than the physical reality warrants. This can happen because they’re distressed and that distress colors their perception. It can also happen because someone who says “I cannot walk through any room in my house” has internalized a subjective experience of overwhelm — even if an outside observer would rate the home as moderately cluttered rather than severely so. The word “clutter” itself activates an emotional response, and that response shapes the answer people give.
The second problem is the mirror image: under-reporting. And this one is arguably more clinically significant. A person who has lived with escalating clutter over many years develops a kind of perceptual adaptation to it. The narrow pathway through the living room becomes “the living room” — it stops registering as a restriction and starts being simply the way the room is. The stacked boxes in the kitchen are part of the landscape. This person might answer “moderate” on a self-report questionnaire about clutter when an independent observer rating the same home would say “severe.” They’re not lying. Their brain has simply recalibrated.
The research team who developed the CIR — led by Dr. Randy Frost of Smith College along with Gail Steketee and David Tolin, published in the Journal of Psychopathology and Behavioral Assessment in 2008 — designed the pictorial scale specifically to solve both of these problems. The elegant insight behind it was this: showing someone an actual photograph of a room at a specific level of clutter bypasses the verbal ambiguity entirely. Instead of asking “would you say your living room is moderately or severely cluttered,” you show someone nine photographs and say, “which one looks most like your living room right now?”
The picture anchors the comparison. It gives everyone the same reference point.
How the Scale Is Actually Structured
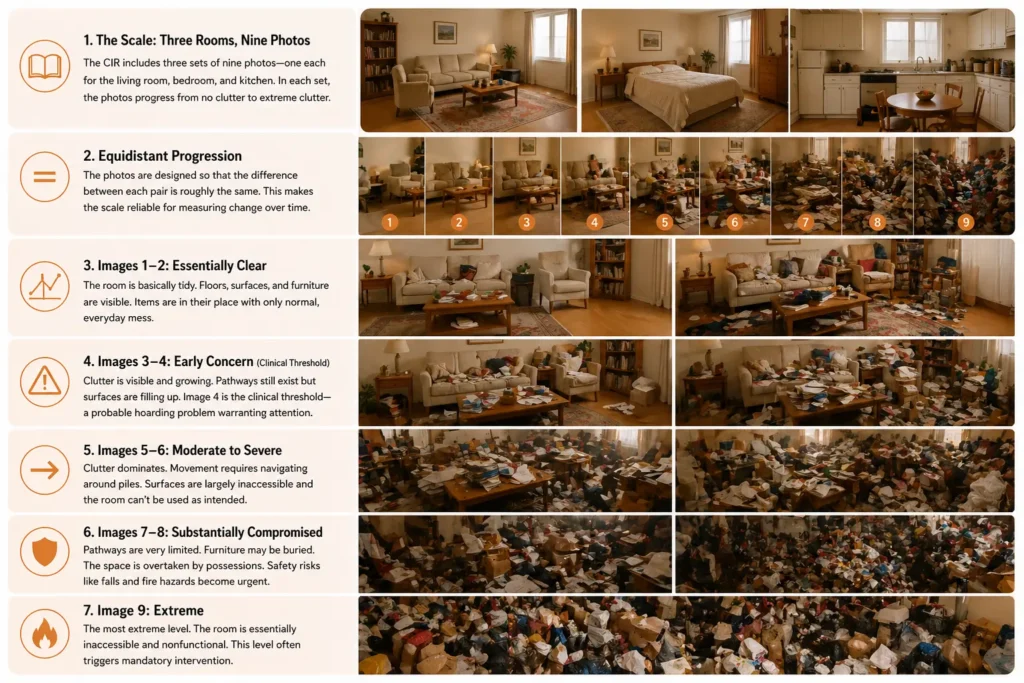
The CIR consists of three separate sets of nine color photographs, one set for each of the three primary rooms that the scale covers: the living room, the bedroom, and the kitchen. Each room gets its own booklet or page of images, and within each set, the nine photographs move along a carefully designed progression from barely any clutter at all to a room that is overwhelmed by possessions.
The critical word there is “equidistant.” The researchers designed the photographs so that the perceived difference between each consecutive image — say, Image 4 and Image 5 — is approximately the same magnitude as the difference between any other consecutive pair. This matters for measurement purposes. If the jump from Image 8 to Image 9 were dramatically larger than the jump from Image 1 to Image 2, the scale would lose its usefulness for tracking change over time. The photographs were selected and validated using a community sample specifically to achieve these roughly equal perceptual intervals.
Here’s what the nine levels look like in practice:
Images 1–2 — The room is essentially clear. You can see the floor, the furniture, the surfaces. Things are in their intended places. There’s normal everyday mess, maybe some items on the coffee table or a jacket on a chair, but nothing that would strike you as unusual or concerning. This looks like most people’s homes on a reasonably organized day.
Images 3–4 — This is where the scale begins to catch things that warrant attention. Clutter is visible and growing. Pathways through the room still exist and are reasonably clear, but surfaces have begun to disappear under accumulated items. There’s a sense of crowding that a visitor would notice. A score of 4 here, according to the International OCD Foundation, represents the clinical threshold: any room rated at Image 4 or higher indicates a probable hoarding problem warranting clinical attention.
That threshold is worth pausing on. Image 4 is not a home that would make the television news. It’s not structurally dangerous. It might not look particularly alarming to someone who hasn’t been trained in hoarding assessment. But the research behind this scale places the clinical line right there — at the point where clutter has begun to meaningfully restrict how a room functions.
Images 5–6 — The clutter is now clearly dominant in the space. Movement through the room requires navigating around piles. Surfaces like countertops and dining tables are largely inaccessible. The room can no longer be used as it was intended without significant workaround. This range typically corresponds to what clinicians would describe as moderate-to-severe hoarding disorder.
Images 7–8 — The room is substantially compromised. Pathways have narrowed to the point where moving through the space is difficult. Furniture may be buried. The volume of possessions has overtaken the human use of the space. Safety concerns — particularly fall hazards and fire risks — begin to emerge as urgent at this level.
Image 9 — The most extreme representation on the scale. The room is filled to a degree that renders it essentially inaccessible and nonfunctional. This corresponds to the most severe presentations of hoarding disorder, the kind that triggers mandatory intervention by social services, fire departments, or housing authorities.
How to Actually Use It
The basic administration is refreshingly simple. A person is given the three pages of photographs and asked to look at the nine images for the first room — let’s say the living room — and identify which image most closely resembles the current state of that room in their home. They circle or record that number, then do the same for the bedroom and the kitchen. The three scores are then averaged to produce what’s called the CIR composite score, which gives a single number representing overall clutter severity across the home.
Scores for people without compulsive hoarding tend to cluster between 1.2 and 1.46 across mid-life samples. Scores for people with hoarding disorder or compulsive hoarding behaviors typically range from 3.64 to 4.5. The numbers are modest-looking, but the differences between them are clinically meaningful.
The tool is designed to be used in several different contexts:
As a self-report completed by the person at home. One of the most powerful features of the CIR is that the self-report version, completed by the person in their therapist’s office or even on their own, has been shown through research to produce results that are significantly correlated with independent clinician ratings done during actual home visits. The original validation study found strong correlations between participant self-report in the clinic and clinician ratings of the CIR in the home (r = 0.74), suggesting individuals with hoarding disorder are able to reliably rate the severity of their clutter when given visual references. This is a big deal clinically, because not every therapist can do a home visit. Not every situation makes a home visit practical. Having a validated tool that allows someone to give an accurate picture of their home from inside a clinic setting opens up assessment to far more people.
As a clinician-administered tool during a home visit. When a home visit is possible, a clinician can complete the CIR independently — looking at each room and selecting the image that best matches what they observe. This clinician-rated version serves as an objective benchmark, particularly valuable when there are questions about the person’s own level of insight into their situation.
As a treatment progress tracker. Because the CIR produces a consistent numerical score over time, it’s extremely useful for measuring whether things are getting better, staying the same, or getting worse. A randomized controlled trial of in-home decluttering augmentation for hoarding disorder, published in BMC Psychiatry, used the blind assessor-rated Clutter Image Rating as one of its primary outcome measures — precisely because it provides a concrete, observable, comparable number that isn’t dependent on how hopeful or discouraged the patient is feeling on any given day.
As a community safety screening tool. Social workers, housing inspectors, adult protective services staff, and fire safety personnel have all adopted versions of the CIR as part of initial assessments when entering a home with suspected hoarding concerns. Rather than describing what they found in vague qualitative terms in their case notes, they can record a CIR score that any other professional can immediately interpret within a shared framework.
The Three-Room Design: A Deliberate Choice
You might wonder why the CIR focuses specifically on the living room, bedroom, and kitchen, and not, say, bathrooms or garages. The answer is partly practical and partly clinical.
These three rooms represent the core functional spaces of daily living — where we rest, eat, and spend our waking hours. The degree to which clutter has invaded these spaces is the most direct indicator of how much daily functioning has been compromised. Garages and basements, by contrast, have a certain cultural permission to be storage areas that the primary living spaces don’t. Clutter in a garage is common and unremarkable. Clutter that’s overtaken the kitchen so you can’t safely cook — that’s a different kind of signal.
There’s also a practical advantage built into the design: the living room photographs can be used to assess other types of rooms in the home that don’t have their own dedicated image sets. If a spare bedroom, an office, or a hallway needs to be assessed, the living room images serve as a reasonable analog.
The Insight Problem — And Why the CIR Partially Solves It
Here is where the science gets genuinely fascinating, and where the CIR’s design reveals just how thoughtfully it was constructed.
One of the cruelest features of hoarding disorder is what clinicians call poor insight — the tendency for people with the condition to significantly underestimate the severity of their own clutter, often without realizing they’re doing so. This isn’t stubbornness or dishonesty. Research has firmly established that it’s a neurological phenomenon.
A landmark study published in Scientific Reports in 2022 examined anosognosia — a clinical term for the brain’s inability to perceive its own deficits — in 71 individuals with DSM-5 hoarding disorder. The researchers found that most participants underrated their clutter when comparing their self-rated CIR scores to independent evaluator ratings done during home visits. And critically, the degree of underrating was correlated with the objective severity of the clutter: the worse the hoarding, the more the person underestimated it. The study also found that underreporting was predicted by altered performance on tests of cognitive control and inhibition, specifically Go/No-Go and Stroop tests. The relation of underreporting to objective clutter suggests that anosognosia may reflect core pathophysiology of the disorder.
In plain English: people with the most severe hoarding were the least likely to recognize how severe it was, and this mismatch was predicted by specific patterns of cognitive difficulty — difficulties that are themselves part of the brain signatures of hoarding disorder. The blindness isn’t random. It’s systematically linked to the severity of the condition itself.
This creates an obvious problem for verbal self-report measures. If someone’s brain is genuinely not registering the full extent of the clutter around them, asking them to describe it in words will produce a significant underestimate. The pictorial CIR helps — but only partially addresses this. The use of a pictorial scale for assessing clutter volume does eliminate the issue of under- or over-reporting based on false associations with the word “clutter.” When given a visual depiction of what different levels of clutter look like, individuals with low levels of insight are provided with a visual comparison that can optimize the accuracy of their response.
The key phrase is “optimize the accuracy.” Not guarantee it. Not fix it entirely. The CIR is a better tool than a purely verbal self-report, but it still relies on the person being able to map their real environment onto a photographic reference — and when insight is severely impaired, even this visual anchor can drift. This is why the clinical recommendation is always to use the CIR alongside other assessment tools, and why a clinician home visit, when possible, provides a more complete picture than self-report alone.
What the Numbers Tell Researchers and Clinicians
A single score is useful. A series of scores collected over time is powerful.
The CIR’s structure makes it uniquely well-suited for tracking longitudinal change — the direction something is moving — which is why it shows up again and again as an outcome measure in treatment studies. When researchers want to know whether cognitive behavioral therapy is actually reducing clutter levels, or whether a community intervention program is making a measurable difference, the CIR gives them a consistent ruler.
In multiple validation studies, the CIR demonstrated strong internal consistency — meaning the scores from the three individual rooms correlate well with each other, not bouncing around randomly. Internal consistency has been demonstrated repeatedly to be high in mid-life samples, with Cronbach’s alpha values ranging from 0.77 to 0.91 across multiple studies. It also showed good test-retest reliability, meaning a person who completes the scale twice within a short time period tends to get similar scores, which is exactly what you want from a measurement instrument.
Interestingly, the CIR was found to be more strongly correlated with measures of clutter specifically than with broader hoarding measures that include difficulty discarding and excessive acquisition. This is actually a feature, not a bug. Clutter is the visible, environmental dimension of hoarding disorder — it’s the thing that can be photographed, observed, and measured by anyone who walks into a home. The CIR measures clutter. Other tools, like the Saving Inventory-Revised (SI-R) or the Hoarding Rating Scale (HRS), measure different dimensions: the emotional difficulty of discarding, the compulsion to acquire, the distress the person feels. A comprehensive clinical picture uses all of these tools together, with each one contributing a different piece of the puzzle.
Think of it like a doctor using several different tests to understand a patient’s health. Blood pressure tells you one thing. Blood glucose tells you something else. Heart rate tells you something different again. No single number is the full picture. The CIR is the blood pressure reading — concrete, observable, and crucial, but not the whole story.
The CIR Across Cultures and Populations
One of the questions that arises with any assessment tool developed in one cultural context is: does it work everywhere? The CIR was originally developed and validated in predominantly Western, English-speaking samples. The photographs themselves were calibrated using a small sample of college undergraduates at the time of their original design — a fact that later researchers pointed out could introduce age and cultural biases into what counts as “equidistant” clutter levels.
Researchers have since tested the tool in other populations. A validation study in BMC Psychiatry examined the CIR in a sample of 500 psychiatric outpatients in Singapore — a markedly different cultural context from the American and European samples used in prior research. The findings were largely supportive: the CIR demonstrated good internal consistency, with good convergent validity with related measures of clutter. The CIR composite score was significantly correlated with all three subscales of the Saving Inventory-Revised, particularly the clutter subscale.
However, the study noted something important: cultural differences in beliefs associated with hoarding — attitudes toward wastefulness, usefulness, and the meaning of objects — are likely to influence both hoarding behavior and the way people respond to photographic comparisons of clutter. The tool works across cultures, but cultural context still matters when interpreting what a given score means.
Similar considerations apply across age groups. A separate study published in International Psychogeriatrics specifically examined whether the CIR holds up in older adults with hoarding disorder, because the original calibration sample was young and perceptions of “normal” clutter levels may differ with age. The findings were reassuring: the CIR appears to be both reliable and valid for assessing clutter levels in older adults diagnosed with hoarding disorder, with similar levels of reliability and validity found in late-life samples as in previous studies conducted in mid-life adults. This matters enormously because older adults are disproportionately affected by hoarding — estimates suggest the rate of hoarding among older adults is approximately three times greater than in the general population — and having a validated tool for this age group is clinically essential.
How the CIR Fits Into the Broader Assessment Toolkit
Because hoarding disorder is multidimensional — it involves clutter, yes, but also difficulty discarding, excessive acquisition, distress, and functional impairment — the CIR is almost never used in isolation by trained clinicians. Instead, it works in concert with a small family of complementary tools.
The Saving Inventory-Revised (SI-R) is a 23-item self-report questionnaire that measures three distinct dimensions: difficulty discarding, clutter, and excessive acquisition. Where the CIR measures the physical environment, the SI-R measures the psychological and behavioral experience. A total score of 40 or higher on the SI-R indicates clinically severe hoarding. Using both together gives you a picture of both the interior experience (how hard is it to throw things away?) and the exterior reality (what does the home actually look like?).
The Hoarding Rating Scale-Interview (HRS-I) is a five-item semi-structured interview — meaning a clinician asks structured questions and probes based on the answers. It covers clutter, difficulty discarding, excessive acquisition, emotional distress, and functional impairment. Each item is rated on a 0-to-8 scale. A total HRS score of 14 or higher indicates clinically significant hoarding, with sensitivity and specificity data from its original validation study supporting this cutoff. The HRS-I takes only about five to ten minutes to administer, making it practical in busy clinical settings.
The Activities of Daily Living in Hoarding (ADL-H) measures functional impairment directly — specifically, how the clutter in the home is affecting the person’s ability to do daily tasks like cooking, bathing, sleeping in their bed, receiving visitors, and accessing emergency exits. Where the CIR tells you how bad the clutter looks, the ADL-H tells you what the clutter is preventing the person from doing. Items are rated on a scale from 1 (“can do easily”) to 5 (“unable to do”), with higher scores indicating greater impairment.
Together, these tools build a comprehensive clinical portrait that words alone could never reliably produce. They turn a subjective description into a measurable profile, and a measurable profile into something you can track over time.
Using It Yourself: What to Keep in Mind
The CIR is freely available through the International OCD Foundation, which hosts downloadable versions of the assessment tool on its clinical resources page (hoarding.iocdf.org). If you’re a family member or caregiver who’s concerned about a loved one’s clutter, looking at those images can be genuinely illuminating — both for helping you understand where things sit on a spectrum, and for providing a non-confrontational way to begin a conversation.
But there are important caveats that deserve honest attention.
First, the CIR measures clutter, not hoarding disorder. These are related but distinct things. A high CIR score suggests that clinical-level clutter is present. It does not, on its own, establish a diagnosis of hoarding disorder. A diagnosis requires assessing the full picture: difficulty discarding, distress, functional impairment, and the ruling out of other explanations. The CIR is a window, not a verdict.
Second, self-administered scores have inherent limitations — especially for the person living in the space. As we discussed at length, the person whose home is being assessed may have perceptual blind spots that limit the accuracy of their own ratings, particularly if their hoarding is more severe. A self-administered CIR score from the person who hoards should be understood as one data point — valuable, but potentially underestimating the actual severity.
Third, how you use the information matters as much as the information itself. The CIR is a clinical instrument designed for assessment and treatment tracking, not for confrontation. If you’ve scored a family member’s home in your head and arrived at a 7 or 8, marching in with that information as a weapon is going to create defensiveness, not change. The research on insight and anosognosia in hoarding disorder makes clear that the person may genuinely not perceive what you perceive — and meeting that gap with compassion, not frustration, is both more humane and more clinically effective.
Why This Simple Tool Matters So Much
It would be easy to underestimate what 27 photographs in three sets of nine actually accomplish. But consider what existed before them: the only way to communicate how bad a home’s clutter was, across professionals, across agencies, across time — was through written descriptions that meant different things to different readers.
“The home is quite cluttered” means one thing to a social worker who has seen 200 homes. It means something different to a housing inspector from a different agency who hasn’t seen this particular home. It means something different again to the person who lives there. Without a shared visual reference, coordination is difficult. Consistent documentation is difficult. And the central goal of clinical care — being able to demonstrate that something is changing — is nearly impossible.
The CIR solved all of that with photographs. Rather than debating whether a home is “messy” or “cluttered,” professionals can point to a specific number that captures the extent of the problem. This consistency helps track treatment progress, justify interventions, and coordinate services between agencies working with the same individual.
One number from 1 to 9. Three rooms. And a conversation that suddenly has something concrete to anchor it.
That’s not a small thing. That’s the difference between a family member saying “Mom, your house is too cluttered” — a statement that can be dismissed, argued with, shrugged off — and a trained professional sitting down with a set of photographs and saying, “Which of these looks most like your living room?” and watching what happens when the person points to Image 6.
Because sometimes — not always, but sometimes — the moment of pointing is also the moment of seeing. And that moment, when it happens, is exactly where treatment begins.
Academic Sources & Further Reading
- “Development and Validation of the Clutter Image Rating” — Frost, Steketee & Tolin, Journal of Psychopathology and Behavioral Assessment (2008). The foundational paper introducing and validating the CIR. Springer Link
- “Validation of the Clutter Image Rating in Older Adults with Hoarding Disorder” — Dozier & Ayers, International Psychogeriatrics (2015). Essential reading for applying the CIR in geriatric populations. PubMed | PMC Full Text
- “Validation of the Clutter Image Rating (CIR) Scale Among Psychiatric Outpatients in Singapore” — Ong et al., BMC Psychiatry (2016). Cross-cultural validation in an Asian psychiatric population. PMC Full Text
- “Anosognosia in Hoarding Disorder Is Predicted by Alterations in Cognitive and Inhibitory Control” — van Roessel et al., Scientific Reports (2022). Groundbreaking study using CIR to measure insight impairment and its neurocognitive predictors. PubMed | PMC Full Text
- “An Objective Measure of Insight in Hoarding Disorder: Associations with Severity, Functioning, and Neuropsychological Performance” — Journal of Psychiatric Research (2025). Replication of the CIR-based anosognosia methodology in Veterans with HD. ScienceDirect
- “A Brief Interview for Assessing Compulsive Hoarding: The Hoarding Rating Scale-Interview” — Tolin, Frost & Steketee, Psychiatry Research (2010). Development and validation of the HRS-I, the CIR’s most frequent clinical companion. PMC Full Text
- “Study Protocol for a Randomized Controlled Trial of In-Home Decluttering Augmentation of Group Cognitive-Behavioral Therapy for Hoarding Disorder: The Joining Forces Trial” — BMC Psychiatry (2023). Example of CIR used as a primary outcome measure in a clinical trial. PMC Full Text
- “Using Virtual Reality in the Inference-Based Treatment of Compulsive Hoarding” — Frontiers in Neuroscience (2016). Example of CIR as a treatment outcome measure in an innovative VR-augmented therapy trial. PMC Full Text
- International OCD Foundation — Clinical Assessment Resources (including free CIR download): hoarding.iocdf.org/professionals/clinical-assessment/
The Clutter Image Rating Scale is available free of charge from the International OCD Foundation at hoarding.iocdf.org. The Saving Inventory-Revised and Hoarding Rating Scale are available at the same resource page. If you are a professional seeking to incorporate these tools into practice, the IOCDF also maintains a directory of hoarding specialists and training resources.